




Telemedicine in some form has existed for decades. The basic premise is fairly intuitive - “I conduct lots of business remotely, why not healthcare?” Despite that, the adoption rate has remained persistently low until very recently and it is largely only used for primary care.

Historically, one barrier to widespread adoption was the lack of reimbursement parity. Insurers would often pay less for remote care on the basis that it cost less to deliver (I’m not paying for an office you don’t need for this visit). Unsurprisingly, providers responded to that incentive and largely avoided telemedicine. Laws requiring “reimbursement parity” have been passed in a growing number of states over the past decade, providing a major catalyst for telemedicine. There’s money it in now.
Concurrently, the ACA pushed up deductibles such that lots of routine care would likely be paid for out of pocket, especially for the younger people who more often go for high deductible plans. If people are paying for care themselves, they start acting like consumers and want to be treated as such. Cost, convenience, and user experience matter more if care is paid for out of pocket and telemedicine fits nicely with that.
Suddenly the pandemic is blowing that up even more and providers are scrambling to move their practices to telemedicine-first or telemedicine-only to provide care while maintaining social distancing. Telemedicine can help keep them and their patients safer than in-person care.
Insurance set the stage and COVID created the urgency.
Telemedicine 1.0: optimizing patients
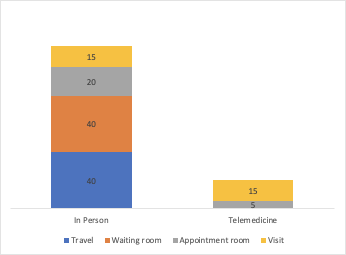
The first, simplest phase of telemedicine largely address problems faced by patients. Getting to a doctor is inconvenient under the best of circumstances and most people aren’t in the best of circumstances. If you live in a dense city and can schedule an appointment, you might reasonably travel 20 minutes each way, hang out in a waiting room for 40 minutes, and sit in an exam room for 20 minutes all for a 15 minute visit with a doctor.
You’ve spent over an hour and a half for a 15 minute visit. That means the total time efficiency of the visit is just a measly 15%. And the real averages are almost all much worse on each of those underlying estimates.
Moving that visit to a phone call means spending less time getting care overall. You could pretty reasonably get to 75% efficiency even if the care you receive is itself unchanged.
The first known telemedicine visit of this type occurred in 1879. The standard operating procedure basically hasn’t changed since then. This is what our health system is rushing to adopt as we try to cope with the pandemic. Other than the phone, the doctor is not using any tools differently than she otherwise would have. The direct cost to her practice is functionally unchanged.
Telemedicine 2.0: optimizing providers
Starting in the 1990s, the internet offered the chance for “store and forward” telemedicine. Store and forward, as the name implies, means information is recorded (stored) and sent (forwarded) to a doctor who then reviews it later. The doctor-patient interaction is “asynchronous” (not at the same time) versus a phone or video call which is synchronous.
Asynchronous is only just now starting taking off, in no small part because of recent changes allowing doctor patient relationships to be established over store and forward (asynchronous) mediums.
This creates opportunities to add more technology to the administration of healthcare, not just the delivery mechanism. Parts of the patient journey like intake forms can be productized without the need for large administrative staffs. Scheduling can largely be obviated for much of routine care if patients and doctors can message asynchronously. If communication is tied directly to medical records systems, charting can be (semi-) automated and data can be originated in structured, machine-readable formats.

Mixing synchronous and asynchronous communications can help practices better triage and allow providers to spend more time with more acute patients. That also means enabling them to spend less time doing the things they hate doing (charting, admin, etc.), the biggest factor in provider burnout.
In all, telemedicine 2.0 takes much fuller advantage of the technology at its disposal. It is healthcare built for telemedicine with the effect of scaling doctors, rather than just trying to port in-person care onto a new medium to make it more convenient for patients. That in turns means making healthcare dramatically more available and affordable.
Telemedicine 3.0: what comes next?
Everything described thus far represents clear advantages to patients and providers but comes with very obvious limitations in both the scope (what can you treat this way) and the benefits (why would you bother). No, we’re never going to eliminate all in-person care nor should we even want to. But even as telemedicine 2.0 makes healthcare more available by optimizing throughput, it still does not fully realize the vision of digital-first healthcare.
That is, the 2.0 scheme is still digitizing and modifying analog practices rather than building digital health tabula rasa and with an eye to the newly possible.
The long term opportunity for telemedicine is not to ignore its limitations (home surgery by an on-demand robot!) or pump vaporware (AI for fully autonomous primary care!) but to provide substantively better outcomes and experiences where it can by doing things that in-person care cannot.
That means taking full (fuller?) advantage of connectivity to do things like passive monitoring to track integrated health and lifestyle data. It means continuous patient monitoring and longitudinal data for both better patient experiences and easier, faster clinical trials. It means unlocking whole new modalities for care delivery and coordination build on top of interoperable medical records (eventually). Imagine all that health data from all those different sources and providers coming together into integrated medical records hubs that can surface conditions or direct patients to care proactively. Missing out on the opportunity to find unexpected issues through more casual patient interactions is a legitimate criticism of telemedicine and will always be part of any sober cost benefit analysis.
It means building adherence and retention directly into patient-facing products and provider-facing tools. It means putting even more process automation behind and products in front of providers to scale knowledge and expertise. It means rather than bolting telemedicine onto a physical world practice, going the other way around to build digital-first full service practices. Imagine starting a patient-provider relationship online and directing a patient to in person care only when necessary and where remote care isn’t enough.
What will all this mean for the health systems’ lock in and pricing power? How will it change the physical and operational needs of providers, and in turn the organization of provider groups? How does the slow shift towards value-based care affect (or even effect) this and vice versa? How will we measure the impacts on individual health? On population health? There is certainly more that we don’t know than what we do.
Whatever digital health 3.0 will look like, it seems clear that that timeline has just gotten pulled forward. It’s happening.
Huge shout out and thank you to Nikhil Krishnan for his excellent post detailing the new HC infrastructure and for giving feedback on this post. If you’re interested in this kind of thing, go subscribe to his newsletter Out Of Pocket.